Newborns
Newborn Care Begins From The Moment Your Baby Arrives
We like to begin newborn care in the hospital and continue as an integral part of the comprehensive care provided by our team whenever possible.
Why choose us?
Our pediatricians and nurse practitioners understand the challenges of taking care of a newborn. They also provide the same gentle care they’d use for treating their family.
If you’re pregnant and looking for a medical home for your newborn, we are accepting new patients.
Who sees my baby at the hospital?
Most of the time we can start our relationship at the hospital when we see your baby soon after birth, but sometimes we begin care after they are discharged from the hospital. We generally see babies in our office 1-2 days after they are discharged from the newborn nursery or NICU.
If you choose our office, be sure to let the hospital know who your pediatrician will be. The hospitals call us after the baby is delivered and we will see you each morning.
One of our physicians will round each morning in the hospital to check on your baby, see how feeding is going, and treat most problems that arise. Most babies are in the hospital 2-3 days and we see them on daily rounds to evaluate how they are feeding, how much weight loss they have, perform a physical exam, and discuss parental concerns.
As mentioned above, we work as a team. Our pediatricians take turns rounding each day, so you may meet several of us during your stay at one of the above hospitals and it may not be the pediatrician you plan to see long term in our office, but we will be sure that person hears all about your baby.
We see newborns at the following hospitals each morning:
- Advent Health -Shawnee Mission
- Overland Park Regional Medical Center
What if you're delivering somewhere else?
If you will be delivering at another hospital, just give us a call after you deliver to schedule your first visit. Please bring any paperwork given on discharge to your first visit. This may include your baby's birth weight, discharge weight, any lab values - such as bilirubin, screening results (such as hearing and cardiac screens) and any other information provided. This can help us learn about the hospital stay and continue care most effectively.
What if your baby needs special care?
We occasionally care for babies in the Newborn Intensive Care Nursery (NICU) if they are there for a short time and for minor issues.
We have a relationship with the Neonatologists (specialists in sick and premature newborn care) at each of the hospitals. They help care for the infants who are requiring more specialized care and let us know when they're ready to see us.
What happens at office visits?
We usually schedule the first visit 1-2 days after discharge. You will need to call to schedule this visit. Due to the nature of our scheduling availability, you may be asked to schedule with a member of our team that you have not yet met, but we think you'll like every one of our physicians and nurse practitioners. All have extensive training and experience and work well together to care for our patient families.
After the first visit newborns usually have several weight checks to be sure they are feeding well and establishing good weight gain. After that, they follow the typical
well visit schedule.
During the visit we will :
- Check your baby’s weight (we check length and head circumference too at standard well visits)
- Ask about your baby’s feeding, bowel, and sleeping habits
- Do a physical examination
- Ask questions about development (in a pre-visit survey- watch for these texts before visits
- Ask if you have questions or concerns about your baby
- Update immunizations as recommended per
our office schedule and standard guidelines
What are newborn screens?
Kansas and Missouri each have routine newborn screens that are done in the hospital or birthing center to identify conditions that can be dangerous when not treated but not easily identified on a physical exam alone. The goal is to identify and treat diseases early enough to prevent serious complications such as growth problems, developmental delays, intellectual disabilities, blindness, deafness, and seizures.
You can learn more about the screenings from:
Who will see my baby?
We work as a team at Pediatric Partners - from the front desk receptionists, to our nursing staff, to our nurse practitioners and pediatricians, we're all here to take the best care of your family!
In the hospital
Our physicians take turns seeing newborns in the hospital. You may get to see a face you already know or meet someone new, but we all trust our work teammates to take great care of our patients.
There are times that newborns require evaluation and care from a neonatologist (specialist in newborn care), such as if your baby is premature, has breathing difficulties, is suspected of an infection, or has need of intensive care. The local neonatologists will update us on how your baby is doing before they go home.
In the office
Newborns are scheduled to see one of our nurse practitioners or pediatricians for each visit. While we know that you will eventually see one of our staff primarily, initially it may be necessary to schedule with another person.
We all trust each other to work within our team, and newborns present the unique circumstance of needing a visit without much notice. Most of our routine well visits are scheduled 2-3 months in advance, so we hold spots for newborns, but it may not be with the person you will choose to see long term. We know this is not ideal because you want to introduce your baby to your chosen practitioner, but we cannot all have newborn spots open or it would cause scheduling issues for all the other patients - including your family long term. While we each have our unique personalities and bedside manners, we all follow standard care guidelines and will take great care of your little one!
If you want to learn more about us, check out the videos we have from each of our pediatricians, about our office locations, general medical advice we give and more.
Learn about each of the physicians and nurse practitioners on our individual pages.
Tongue Tie Management
WHEN THE TONGUE'S MOVEMENT AFFECTS FEEDING, A FRENOTOMY MAY BE RECOMMENDED
Some babies are born with a short frenulum under the tongue. This inhibits the baby from extending the tongue past the lips.
Many people refer to this condition as "tongue-tied" (medically called ankyloglossia).
The tongue’s frenulum attaches the tongue to the floor of the mouth. It should allow the tongue to extend past the lower gums and lip, elevate to the roof of the mouth, and move from side to side. If it is too thick, too short, or too far toward the tip of the tongue it can affect feeding, speech, tooth placement, and growth of the mouth.
Not all frenulums that appear thick need to be treated. If the tongue functions well and the baby is feeding successfully, we do not need to do any procedures. Dr. Stuppy has written a summary of the guidelines recommended by otolaryngolosts (ear, nose, and throat specialists) on management of tongue, lip, and cheek ties that you can read here.
Tongue tie affects about 4 in 100 people. It is more common in boys and there often is a family history of tongue tie.
HOW IS IT TREATED?
Treatment of tongue tie involves lifting the tongue and clipping the frenulum (frenotomy).
A frenotomy can be done by trained pediatricians, ENTs, or dentists. Some of our pediatricians have this training, so if you're concerned we can make sure you get scheduled with one of them for an evaluation. There are local dentists who do a laser procedure, but this is more expensive and has not been shown to offer any benefit. (See Dr. Stuppy's review of guidelines for more details.)
The frenulum does not have nerves for pain, and most newborns tolerate the procedure well without any anesthetic. We usually ask that they feed immediately after the procedure to assess their feeding.
It is recommended if the frenulum is very thick, posterior, very vascular or if there is a family history of bleeding disorders that an ENT specialist does the procedure.
Alternates to frenotomy:
- Work with lactation to improve latch
- Work with a speech pathologist or occupational therapist for feeding therapy
Risks of clipping:
- Infection
- Bleeding (usually minor)
- Swallowed blood can lead to spitting up
- Damage to salivary glands (rare)
- Need for more surgery
- Feeding aversion
After the clipping the underside of the tongue will get a yellowed area (called "granulation tissue"). This is the normal healing tissue and will resolve within a few days.
PHOTOS FROM STANFORD.EDU


The pictures are the same baby before and after the frenulum was clipped.
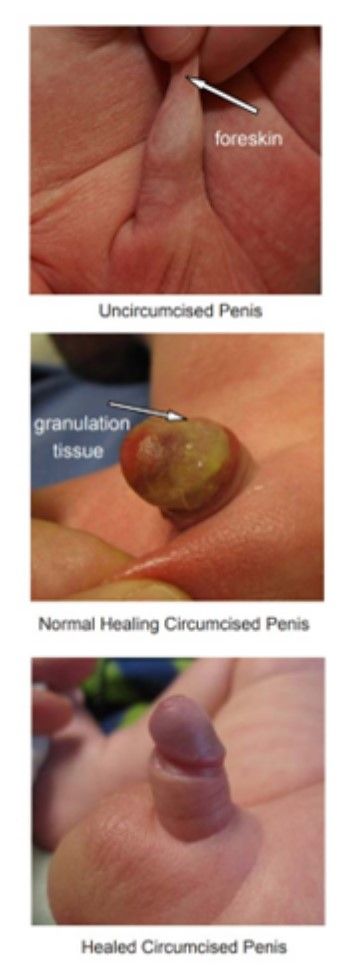
Care of the Penis - circumcised and uncircumcised
Uncircumcised penis
The foreskin is attached to the head of the penis at birth and will usually naturally pull away over the first few years of life. A white substance may be seen as the foreskin pulls back. This is smegma and normal, not a sign of infection.
As long as the foreskin doesn’t easily retract, only the outside skin needs to be cleaned.
If the foreskin retracts a little, clean only the exposed area with water. Don’t use soap on this area - this can irritate the skin. After cleaning always replace the foreskin back over the head of the penis.
As your child gets older and the foreskin has completely separated and retracts easily, begin to teach him to clean underneath it as he bathes.
If the foreskin does not naturally pull away from the head of the penis an this causes painful erections, bring your child in for an evaluation of the situation.
Circumcision types and care
There are two main types of circumcision, one that leaves a plastic ring (Plastibell) on the head of the penis, and another that removes the foreskin and is left open with petrolatum jelly on gauze.
Care depends on the procedure done. After a baby's circumcision, it takes about a week to heal regardless of the method used.
After the healing has taken place, no special care is needed other than routine cleaning.
A WORD ABOUT ADHESIONS...
Sometimes the penis will sink into the fat pad surrounding it, allowing the skin to reattach over time.
If your child's foreskin comes back over the head of the penis, push back on the fat pad to pull the skin off the head of the penis with diaper changes. Apply petrolatum jelly (Vaseline) to the area to prevent sticking.
If it does stick, it is called an adhesion. This usually doesn't cause any problems - remember that uncircumcised penises generally pull away from the foreskin over the pre-pubertal years. The adhesions of a circumcised penis will also naturally pull away over time. If they cause pain, they should be addressed.
A white substance called smegma sometimes is seen around the edges of the head of the penis. This looks like cottage cheese and is sometimes mistaken for pus. It is not pus and is a normal substance made by the penis. Gentle removal with a moist cloth is all that's needed if it's bothersome.
PROCEDURE DESCRIPTIONS
The type of procedure done is dependent on the training and experience of the person performing the procedure. Risks and benefits overall are similar. The final "look" of the penis will be the same after the first week.
Both types use a local anesthetic called lidocaine to numb the area. This injection may sting initially (sugar and a pacifier are used to help pain control for the sting) and the injection may leave a bruise at the base of the penis. Babies can still feel the cold of the cleaning product we use to decrease risk of infection and they can still feel tugging, but the sharp pains of the procedure are lessened with the lidocaine. The foreskin is pulled away from the head of the penis (aka glans).
The remainder of the procedure done and aftercare depends on the type of circumcision.
MOGEN CLAMP:
After the Mogen Clamp it will look bright red and swollen initially, then less swollen. As it heals, yellow granulation tissue appears on the head of the penis. This is normal and NOT an infection.
We recommend putting petroleum jelly on the head of the penis during the healing process to keep it from sticking to the diaper. If stool gets to the area, simply rinse with water without rubbing the area much. Reapply petroleum jelly each diaper change. We suggest you do not use any creamy products or lotions on the healing penis, as they cause irritation.
- The foreskin is pulled up and the clamp is placed over the glans, to protect it from being cut.
- The clamp puts pressure on the tissues to prevent bleeding.
- The foreskin above the clamp is removed.
- No stitches are needed unless there is excessive bleeding, which is a rare complication.
- The head of the penis will look open and raw during the healing process. This is normal!
- Change the gauze pad with petrolatum jelly (Vaseline) with diaper changes since it will be soiled.
- Rinse the head of the penis with water if stool (poop, bowel movement, meconium) gets on it, but usually simply changing the gauze is sufficient.
- Continue to place Vaseline gauze on the head of the penis until it is healed. You will know when it is healed when there are no more red or yellow areas.
- If there are signs of infection, such as redness of the penis shaft, temperature over 100.4F, poor feeding or fussiness, your baby should be evaluated.
PLASTIBELL
- A plastic ring (Plastibell) is inserted between the head of the penis and the foreskin and tied off.
- The ring is left in place until it falls off naturally, generally 3-7 days later.
- Routine cleaning with diaper changes is done.
- If the ring does not fall off within 14 days or if it slips down the shaft of the penis, bring your baby in to be evaluated. This is an emergency if it seems red, tender, or your baby has a temperature over 100.5F, is fussy or not feeding well.
Recommended Newborn Resources
Milestone Tracking and Tools to Maximize Your Child's Development
- Track your child's development with FREE online tools.
- Find developmental milestone information so you can keep track at home.
- Pathways offers resources for infant and child development.
- Zero to Three offers resources for infant and child development and parenting.
- Did you know you can sign up for free weekly texts coinciding with your due date to help with every stage of pregnancy and the baby's first year? Visit text4baby for more details.
Local Resources to Optimize Development
- Parents As Teachers works with parents to teach them how to teach their infants through 3 year olds.
- Infant and Toddler Services provides therapies for Kansas infants and toddlers through 3 years of age with delays in developmental skills, such as speech and language or gross motor skills.
- First Steps provides therapies for Missouri infants and toddlers through 3 years of age with developmental delays.
Colic (Fussy baby) Resources:
- Period of Purple Crying http://purplecrying.info/
- All Babies Cry https://www.allbabiescry.com/
Daycare:
Childcare can be done in a person's home or in an established child care center. There are pros and cons to each, so consider your family's needs to start your search.
ChildCare Aware has a searchable database to help locate childcare providers, check licensing of childcare providers and see inspection reports. Click on the state to find providers in Kansas and Missouri.
To help locate a childcare provider, learn how to find the best childcare, and more use this searchable database: Childcare.gov. Use their Tip Sheets to help find the best care for your child(ren).
Related pages for more information:
Services


